

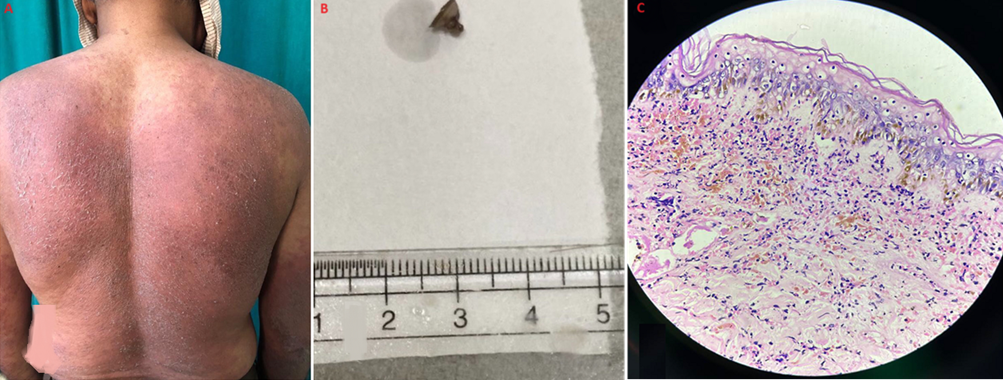
Visualizing drug-induced Stevens-Johnson syndrome: a clinical image
Shivali Kalode, Prerna Tekulwar
PAMJ. 2024; 48:183. Published 19 Aug 2024 | doi:10.11604/pamj.2024.48.183.44544
Corresponding author
Shivali Kalode, Department of Pathology, Jawaharlal Nehru Medical College, Datta Meghe Institute of Higher Education and Research, Sawangi (Meghe), Wardha, Maharashtra, India (shiv.tin143@gmail.com)
This image
| Articles published in JOURNAL_ABBREVIATION are Open Access and distributed under the terms of the Creative Commons Attribution 4.0 International (CC BY 4.0). |  |

eISSN: 1937-8688
The Pan African Medical Journal (ISSN: 1937-8688) is a subsidiary of the Pan African Medical Journal. The contents of this journal is intended exclusively for professionals in the medical, paramedical and public health and other health sectors.
Currently tracked by: DOAJ, AIM, Google Scholar, AJOL, EBSCO, Scopus, Embase, IC, HINARI, Global Health, PubMed Central, PubMed/Medline, ESCI
Physical address: "Kenya: 3rd Floor, Park Suite Building, Parkland Road, Nairobi. PoBox 38583-00100, tel: +254 (0)20-520-4356 | Cameroon: Immeuble TechnoPark Essos, Yaounde, PoBox: 10020 Yaounde, tel: +237 (0)24-309-5880"
PAMJ
Primary Health Care Practice Journal
African Journal of Health Economics, Systems and Policy
PAMJ Conference Management System

About PAMJ - Manuscript Hut™
The Manuscript Hut is a product of the PAMJ Center for Public health Research and Information.
Kenya: 3rd Floor, Park Suite Building, Parkland Road, Nairobi. PoBox 38583-00100, tel: +254 (0)20-520-4356
Cameroon: Immeuble TechnoPark Essos, Yaounde, PoBox: 10020 Yaounde, tel: +237 (0)24-309-5880
Copyright © - Pan African Medical Journal - CEPHRI (Kenya). 2026
PAMJ One Manuscript Hut - (MMS V.4.0). Release date April 2026 - Customized for PAMJ.
For advertisers Contact the PAMJ sales service. Download our latest media-kit.
sales-service@panafrican-med-journal.com
 |